





Even in an age dominated by digital monitors, Korotkoff
sounds remain the clinical gold standard, especially in hospitals and
diagnostic settings.
At AarogyaaBharat.com, we aim to explain not just what
happens, but why it happens clearly and practically.
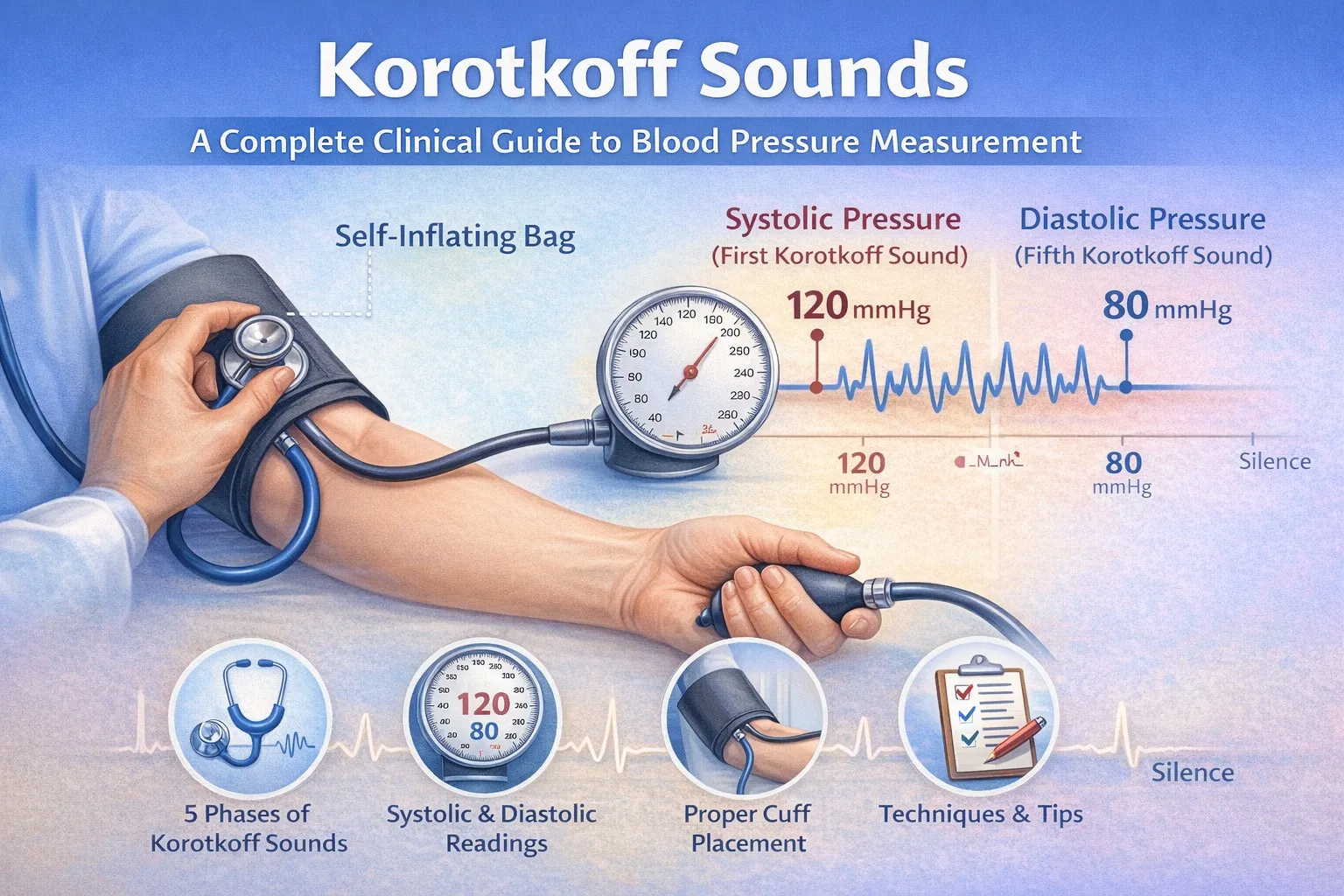
What Are Korotkoff Sounds?
Korotkoff sounds are the sounds produced when blood flows
through a partially compressed artery during gradual deflation of a blood
pressure cuff.
They were first described in 1905 by Dr. Nikolai Korotkoff,
a Russian physician, and remain central to cardiovascular assessment today.
These sounds are caused by:
- Intermittent
arterial opening
- Turbulent
blood flow
- Vibration
of the arterial wall
The Physiology Behind Korotkoff Sounds
Understanding the physiology makes BP measurement far more meaningful.
When the cuff pressure is:
- Above
systolic pressure → artery fully closed → no blood flow, no sound
- Between
systolic and diastolic pressure → artery opens intermittently → turbulent
flow, sounds heard
- Below
diastolic pressure → artery fully open → laminar flow, silence
Turbulence = sound
Laminar flow = silence
The Five Phases of Korotkoff Sounds (With Clinical
Meaning)
Phase I – Clear Tapping Sounds
- First
appearance of repetitive tapping
- Marks
systolic blood pressure
- Clinically
the most important starting point
Phase II – Swishing or Murmuring Sounds
- Softer,
longer sounds
- Represents
partially compressed artery
- Can
be affected by auscultatory gap
Phase III – Loud, Crisp Sounds
- Sharper
and louder
- Increased
blood flow through artery
- Indicates
improving arterial patency
Phase IV – Muffling of Sounds
- Sounds
become softer and dull
- Sometimes
used as diastolic BP in:
- Children
- Pregnant women
Phase V – Disappearance of Sounds
- Complete
silence
- Standard
marker for diastolic blood pressure in adults
What Is the Auscultatory Gap? (Very Important)
An auscultatory gap is a temporary disappearance of
Korotkoff sounds between Phase I and Phase II.
Why it matters:
- Can
lead to false low systolic BP
- Common
in elderly patients and those with hypertension
- Prevented
by palpating systolic pressure before auscultation
This is a key reason clinician are trained carefully in
manual BP measurement.
Clinical Importance of Korotkoff Sounds
Korotkoff sounds help clinicians:
- Diagnose
hypertension accurately
- Monitor
treatment effectiveness
- Detect
vascular stiffness
- Identify
irregular heart rhythms
- Avoid
errors caused by faulty devices
In ICUs and cardiology clinics, manual BP measurement is
often preferred.
Manual BP vs Digital BP: Clinical Perspective
|
Aspect |
Manual BP
(Korotkoff) |
Digital BP |
|
Accuracy |
High (trained
user) |
Variable |
|
Detects
arrhythmia |
Yes |
Often no |
|
Hospital use |
Preferred |
Limited |
|
Skill
required |
Yes |
Minimal |
Digital devices are convenient - Korotkoff sounds are
definitive.
Common Errors That Distort Korotkoff Sounds
Errors often arise from:
- Incorrect
cuff size
- Cuff
over clothing
- Rapid
deflation (>2–3 mmHg/sec)
- Poor
stethoscope positioning
- Talking
or movement during measurement
Correct technique is as important as correct equipment.
Special Clinical Situations
- Children:
Phase IV may be preferred
- Pregnancy:
Phase V may be absent
- Atrial
fibrillation: Sounds irregular; multiple readings needed
- Shock:
Sounds may be faint or absent
Clinical judgment is essential.
How Aarogyaa Bharat Supports Accurate BP Measurement
At Aarogyaa Bharat, we support cardiovascular accuracy by
providing:
- Clinically
reliable BP monitors
- Correct
cuff sizes for all patients
- Educational
resources for healthcare teams
- Trusted
medical guidance
We believe accurate measurement is the foundation of correct treatment.
Conclusion
Korotkoff sounds remain one of the most elegant and reliable
tools in clinical medicine.
They convert subtle blood flow changes into audible signals that guide life-saving
decisions.
In a world of automation, they remind us that good medicine
still begins with careful listening.
For trusted medical education and healthcare solutions, Aarogyaa Bharat is always with you.






